

Consent to an in-person consultation and/or to have Dr. Sandeep Sattur/Dr. Indu Sattur and/or his/her staff (hereinafter collectively “my Doctor”) perform medical procedures, whether regarded as necessary, elective, or aesthetic, on and from the date of this COVID-19 Informed Consent Agreement For In-Person Consultation (“Consent”) and at any time thereafter. I am aware that exposure to COVID-19 can result in severe illness, intensive therapies, extended intubation and/or ventilator support, and even death. I am also aware of the possibility that the procedure itself, whether performed in my Doctor’s office or in a hospital, may result in a more severe case of COVID-19 than I might have had without the procedure.
I also understand in-person consultations and/or having my procedure performed at this time increases the risk of my transmission of COVID-19 to my Doctor. To reduce the possibility of COVID-19 exposure or transmission at my Doctor’s office, I accept that my Doctor will implement infection-control procedures with which I must comply, before, during, and after my consultation and/or procedure, for my own protection as well as that of my Doctor.
I have informed my Doctor of any COVID-19 testing I or any person living with me during the past 14 days has received, as well as the results of that testing, and if I am tested between now and the date of my procedure, I will immediately provide the results of that testing to my Doctor.
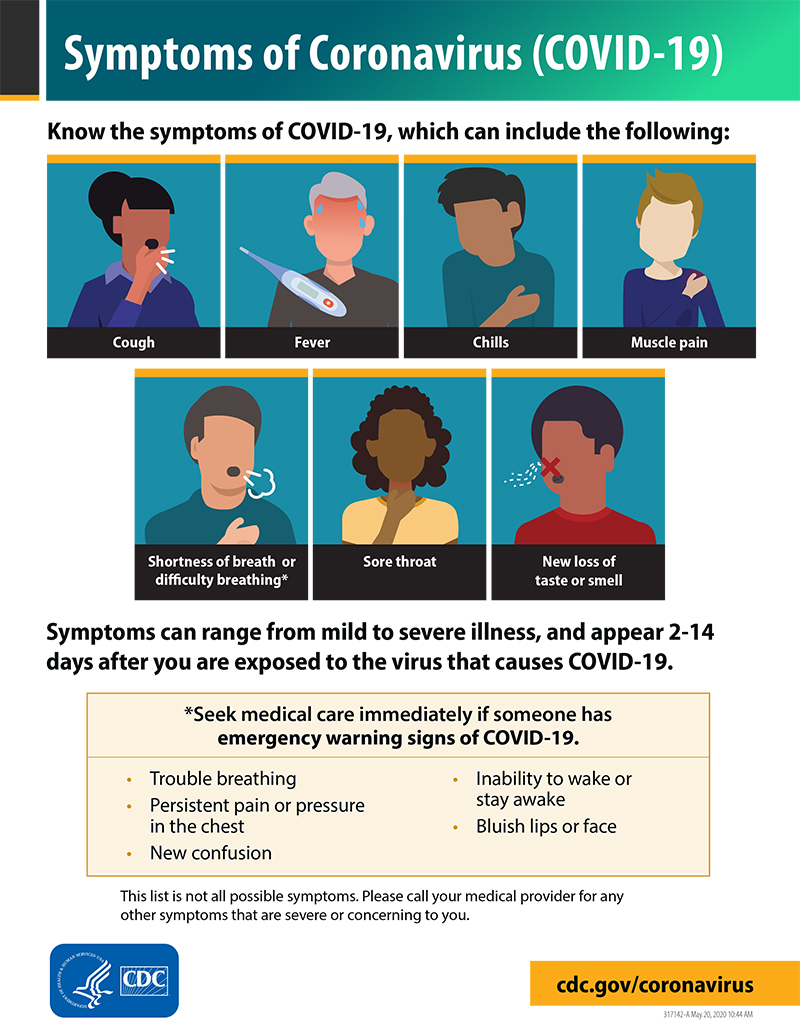
I confirm neither I nor any individual living with me has any of the COVID-19 symptoms listed by the Centers for Disease Control https://www.cdc.gov/coronavirus/2019-ncov/downloads/COVID19-symptoms.pdf, which website I have consulted; neither I nor any individual living with me during the past 14 days has experienced any such symptoms; and that I and all persons living with me for the past 14 days have practiced all personal hygiene, social distancing and other COVID-19 recommendations contained within all governmental orders issued by my city and state. I undertake to honestly disclose this information and any other information which I feel is necessary to enable my Doctor to make a clinical decision and to avoid putting myself and others at risk.
Your Responsibility to Minimize Your Exposure
To obtain in-person consultation, I agree to take certain precautions which will help keep everyone (me, the Doctors, our respective families, and other patients) safer from exposure, sickness, and possible death.
I agree to undertake each of the actions listed below:
- I will only keep my in-person appointment if I am symptom-free.
- I will take my temperature before coming to each appointment. If it is elevated (100 Fahrenheit or more), or if I have other symptoms of the coronavirus, I agree to cancel the appointment or proceed using telemedicine.
- I will wash my hands or use alcohol-based hand sanitizer when I enter the clinic.
- I will adhere to the safe distancing precautions the Doctors have set up in the waiting room and consulting room
- I will wear a mask in all areas of the clinic.
- I will keep a distance of 6 feet and there will be no physical contact (e.g. no shaking hands) with the doctors or staff.
- I will try not to touch my face or eyes with my hands. If I do, I will immediately wash or sanitize my hands.
- I will be coming alone to the clinic. If a relative is accompanying me, I will make sure I inform the Doctors before your appointment so seating arrangements could be made keeping safe distancing. Only one relative or accompanying person with the patient will be permitted inside the clinic.
- I will take steps between appointments to minimize my exposure to COVID.
- If I have a job that exposes me to other people who are infected, I will immediately let the doctors and the staff at the clinic know.
- If my commute or other responsibilities or activities put me in close contact with others (beyond your family), I will let doctors and the staff at the clinic know.
- If a resident of my home tests positive for the infection, I will immediately let doctors and the staff at the clinic know and the Doctors will then begin/resume treatment via telemedicine.
The Doctors may change the above precautions if additional local, state, or national orders or guidelines are published.
All topics above have been discussed with me, and all my questions have been answered to my satisfaction. Being fully informed, I accept the risk of COVID-19 exposure and I will bear the cost of any COVID-19 treatments required. I have been given the opportunity to postpone my in-person consultation and/or procedure until the COVID-19 pandemic is less prevalent, but I choose to have my in-person consultation and/or procedure performed now. If I am the parent, guardian, or conservator of the patient, I am legally able to provide this consent on his/her behalf. I have read this Consent and am authorized to consent on the patient’s behalf. All information provided by me to my Doctor, including in this Consent, is true and accurate.